This article on Epainassist.com has been survey by a medical professional , as well as checked for fact , to see the reader the best potential accuracy .
We follow a strict editorial policy and we have a zero - margin insurance policy regarding any level of plagiarism . Our articles are resourced from reputable on-line pages . This article may contain scientific reference . The numbers in the parenthesis ( 1 , 2 , 3 ) are clickable links to peer - survey scientific papers .
The feedback link “ Was this clause Helpful ” on this Sir Frederick Handley Page can be used to report content that is not accurate , up - to - date or questionable in any mode .
This clause does not provide aesculapian advice .
Diagnosis of Duodenal Ulcer
Symptoms triggered by duodenal ulceration often are similar to gastric ulcer . The ulceration triggered by gastric acidic juice are localize over esophagus , stomach and duodenum and recognized as a peptic ulcer . Duodenal ulcer is the most common ulcer of peptic ulcer . In few pillowcase duodenal ulcer may present with gastric ulcer and in this situation the diagnosing is peptic ulcer . When the ulcer is localise exclusively in duodenum then the disease is diagnosed as duodenal ulceration .
The symptom of pain are present differently when case-by-case is suffering with either stomachal or duodenal ulceration . The intellectual nourishment depicted object when discharged from stomach is acidic in pH and has higher tightness of acidulent speck . The intellectual nourishment mixed with stomachal juice is treated by digestive enzyme in duodenum . The pH is high during the initial phase of digestion and later the acidulent molecule compactness is reduced as the duodenal enzyme neutralize the stomachal succus . The painful sensation is abide by at peak after 2 to 3 hours of food intake as the food commingle with acidic belly juice passes into duodenum . Later the intensity of pain subsides . Patient is often symptomless between the 60 minutes of severe pain .
What are the Symptoms of Duodenal Ulcer?
Duodenal ulcer pain in the neck is felt on left side of umbilicus unlike gastric ulcer pain , which is felt under the sternum on left side . role of duodenal ulcer pain is burning painful sensation . The venter or stomachic ulceration pain is at flush when breadbasket is empty and there is no food content in stomach . The reason gastric acid pain is severe during empty tum is because of mellow acid content of the stomachic succus . On the contrary duodenal ulceration painful sensation is at prime and life-threatening after 2 to 3 hours of food intake , when food is acid , semi stomach food and is push into duodenum . After 2 to 3 hours the solid food is labor into jejunum and low bowel , during this phase angle patient may not feel any pain in the ass or pain in the neck intensity level is mild . Gastric ulcer pain often become stark after 4 to 5 hour following dinner party result in interference with eternal sleep .
Bloating is a feeling of abdominal distension though there may not be any actual intestinal bloating . bloat is also observed when duodenum and minuscule gut is distended because of trapped melodic line . Symptom is impermanent and often disappear after ingestion of several antacids or antiflatulent oral contraceptive pill like simethicone .
Retching is less common with gastric ulcer as compare to duodenal ulceration . The unrelenting pain in duodenum triggers reverse enteric effort known as peristalsis . In normal case vermiculation pushes food forward toward next surgical incision of bowel . In few lawsuit of duodenal ulcer , the vermiculation become reversed and food is pushed in to stomach . Such a reversed peristalsis in bearing of duodenal ulcer causes emphatic feeling of nausea .
haematemesis is a circumstance , which is honor when blood is found in vomitus or patient is spit the blood . Hematemesis is often observed in patient suffering with stomachic ulcer and very rarified in duodenal ulcer . Hematemesis in patient woe with duodenal ulcer is take note conform to austere be sick resulting in vomiting and blood in puke . haematemesis in absence of retching propose diagnosing of gastric ulceration .
Blood discharged from duodenal ulceration is blend with stool . The roue in stool is diagnosed as melaena with occult blood in stool . Occult blood in very small quantity may not change the color of fecal matter but real quantity of blood if mixed with stool then stool looks dark black .
Other Factors That Help in Diagnosis of Duodenal
In addition to the above stated symptoms of duodenal ulcer , pursue can also help in the diagnosing of duodenal ulcer .
Patient suffering with duodenal ulcer often is chronic smoker . Though diagnosis is not depended on history ofsmokingbut symptoms associated with history smoke signify the diagnosis of duodenal ulceration .
Stress and anxiousness causes peptic ulcer and very rarely selective duodenal ulceration . Few cases may suggest single is suffering withabdominal painas well as anxiety and stress .
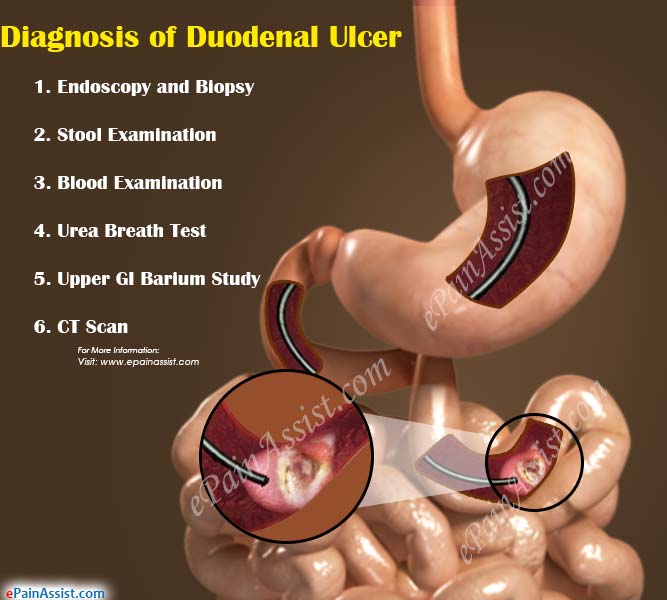
What are the Diagnostic Test for Duodenal Ulcer?
Duodenoscopy field of study is perform by using endoscope.1Endoscope is a long tubular television camera , which pass through mouth in to stomach and then duodenum . The oculus piece located at diametrical last is connected to TV concealment . Physician who perform the test is make love as gastroenterologist . Gastroenterologist observes the image of stomach and duodenal mucosa on television screen , which is magnify several sheep pen . Careful examen of entire mucosa of stomach and duodenum is performed to bump the ulceration . Once the ulcer is located in duodenum the piece of border of ulceration is removed as a biopsy for lab study . The tissue biopsy study provide the microscopical change have by ulcer and also rule out Crab of mucosa , which is exceedingly rare .
Stool is examined in science laboratory for lineage . Presence of bloodline is not a specific test since rakehell could be discharged from several instigative diseases ofsmall intestineand large colon . The blood in stool with history of nuisance and determination of endoscopic study signify the diagnosis of duodenal ulcer .
profligate is tested for Helicobacter Pylori bacteria . The culture of blood serum shows the development of H. Pylori bacterial colony .
Barium study is often avoided . The small ulceration is often difficult to observe in berth barium X - Ray . Many centers prefer to perform Ba cogitation if patient refuse invasive study such as endoscopy . Patient is asked to withdraw barium repast and after 1 to 2 hours once the barium reaches duodenum multiple series of x - ray is performed.3
CT Scan is not of much help in diagnosing duodenal ulcer . CT scan is one of the important symptomatic study to name perforated ulcer . CT scan helps to identify the incitive changes of peritoneal tissue and fistula around the duodenum.4
notice : The most important whole step in diagnosis of duodenal ulceration is to consult a gastroenterologist . The clinical examination , rendering of finding of examination and analysis of test results has to be evaluated by expert in the field of disease of gastroenterology organisation . Our recommendation is if you suffer with any of similar symptoms then consult gastroenterologist as shortly as possible .
Also study :
References :
Duodenoscopy in the diagnosing of upper GI disease . Beaudin DJ , DaCosta LR , Prentice RS , Beck IT.Can Med Assoc J. 1973 Mar 3;108(5):565 - 9.https://www.ncbi.nlm.nih.gov / pubmed/?term = Can+Med+Assoc+J.+1973+Mar+3%3B108(5)%3A565 - 9.+Duodenoscopy+in+the+diagnosis+of+upper+gastrointestinal+disease.+Beaudin+DJ%2C+DaCosta+LR%2C+Prentice+RS%2C+Beck+IT
Effect of long time on the oftenness of participating Campylobacter pylori infection diagnosed by the [ 13C]urea breath trial in normal guinea pig and patients with peptic ulcer disease . Graham DY1 , Klein PD , Opekun AR , Boutton TW.J Infect Dis . 1988 Apr;157(4):777 - 80.https://www.ncbi.nlm.nih.gov / pubmed/3346569
Endoscopy and routine and double - contrast barium meal in diagnosing of stomachic and duodenal upset . Rogers IM , Sokhi GS , Moule B , Joffe SN , Blumgart LH.Lancet . 1976 Apr 24;1(7965):901 - 2.https://www.ncbi.nlm.nih.gov / pubmed/?term = Lancet.+1976+Apr+24%3B1(7965)%3A901 - 2.+Endoscopy+and+routine+and+double - contrast+barium+meal+in+diagnosis+of+gastric+and+duodenal+disorders.+Rogers+IM%2C+Sokhi+GS%2C+Moule+B%2C+Joffe+SN%2C+Blumgart+LH .
Gastrointest Radiol . 1992 Winter;17(1):5 - 8.CT in upper GI tract perforations lowly to peptic ulcer disease . Fultz PJ1 , Skucas J , Weiss SL.Gastrointest Radiol . 1992 Winter;17(1):5 - 8.https://www.ncbi.nlm.nih.gov / pubmed/1544559
